|
|
|
|
| A Critical Care Scenario |
|
A fifty-nine year old man presents with 5kg weight loss and jaundice,
a carcinoma of the head of pancreas is diagnosed,
and he is admitted for a Whipple's procedure.
He is still mildly jaundiced, but has gained a little weight following
endoscopic placement of a biliary stent.
He has no other significant past medical history, and specifically no
history of palpitations.
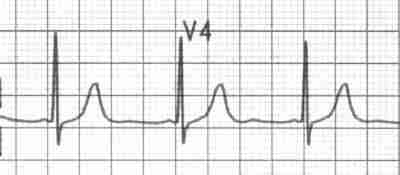
Following the 4.5 hour procedure he initially does well, but has to return to theatre for massive intra-abdominal bleeding. A bleeding vessel is ligated. Seven units of blood are transfused, and he is returned to ICU intubated. Again stable in all respects, well-analgesed with patient-controlled analgesia, and maintaining good oxygenation on an FiO2 of 0.4, he is soon extubated. Half an hour later, he develops intermittent runs of tachycardia (up to a rate of 160/min), which progressively become more frequent, and then continuous. Blood pressure is maintained. Carotid sinus massage transiently breaks the arrhythmia, which then recurs. Arterial blood gas analysis is within normal limits, as are serum electrolytes, including magnesium and potassium. His pain is still well-controlled. Because such arrhythmias are often self-limiting, and he is haemodynamically stable, he is observed for one hour, but the rhythm disturbance doesn't settle. What would you do now?
|
Cordarone, Cordarone X.
Also: Amiodar, Ancoron, Angiodarona, Atlansil,
Cordarex, Miocard, Miodaron, Ortacrone, Ritmocardyl, Rythmarone, Trangorex.
Strong Contra-indications include:
As a minimum we recommend:
Long term monitoring and precautions should probably include:
Common interactions:
Other interactions:
Histologically or in sputum lamellar inclusion bodies are said by some to be specific for amiodarone cytotoxicity; this is probably not true [ Kennedy JI, Clin Chest Med 1990 Mar;11(1):119-29 ], as many patients on amiodarone will have lamellar bodies and foamy macrophages, whether they have pulmonary toxicity or not [Hum Pathol 1987 Apr;18(4):349-54 ]. There is an increase in lung CD8-positive cytotoxic lymphocytes, as well as neutrophils and "foamy" macrophages. LDH levels may be raised. Gallium scanning may be of value in identifying this disorder.
Amiodarone has actions in classes I,II,III and IV of the Vaughan Williams
classification, but is predominantly a membrane stabilizer (class III).
Its class III action is mediated by inhibition of the rapid component of
the delayed potassium rectifier IKr (as with sotalol) but also an effect
on the slow component. It is the latter effect that probably explains why
amiodarone only minimally increases the risk of torsades de point (polymorphic
ventricular tachycardia), unlike sotalol.
Desethylamiodarone alters gene expression, antagonising the effects
of T3! [ J Cardiovasc Pharmacol 1998 Oct;32(4):654-61 ]
 Amiodarone is a white powder derived from benzofuran, and has a molecular
weight of 645.32, C 25 H 29 I 2 NO 3 ,
usually presented as a hydrochloride (MW 681.8);
it is not very soluble in water, and is very lipophilic.
Amiodarone is a white powder derived from benzofuran, and has a molecular
weight of 645.32, C 25 H 29 I 2 NO 3 ,
usually presented as a hydrochloride (MW 681.8);
it is not very soluble in water, and is very lipophilic.
Amiodarone for intravenous use is solubilized using polysorbate 80 This vehicle causes hypotension, decreases heart rate, depresses AV nodal conduction and increases atrial and ventricular myocardial refractory period!
The following brief notes are far from complete!
Class III antiarrhythmics such as amiodarone have gained favour following the (disastrous!) CAST trial of class I agents. Investigational agents with class III activity include azimilide, dofetilide, dronedarone, ersentilide, ibutilide, tedisamil, and trecetilide [ J Cardiovasc Electrophysiol 1999 Feb;10(2):307-17 ]
Information on this page is provided for teaching purposes. You should not make a clinical treatment decision based on information contained in this page without consulting other references including the package insert of the drug, textbooks and where relevant, expert opinion. We cannot be held responsible for any errors you make in administering drugs mentioned on this page, nor for use of any erroneous information contained on this page.
| Date of First Publication: 22 April 1999 | Date of Last Update: 2006/10/24 | Web page author: Click here |