It's important to note that substantial portions of the aorta, especially
the arch, are not visualised using TEE. In addition, fine detail may
be poorly seen, especially where the probe is very close to the
aortic wall. For these reasons, expensive epiaortic scanning probes
(that usually function at about 10 MHz, compared with the 4 to 7 MHz of
most TEE probes) are often used to identify atheroma prior to aortic
cannulation during cardiopulmonary bypass surgery.
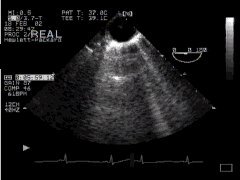
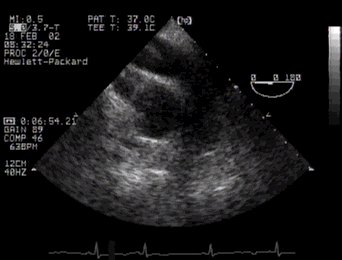
1. Descending AortaIt is easy to imagine the circular image of the descending aorta seen in short axis view when the TEE probe is inserted to about 40cm and turned slightly left. Here it is - 'DESC Aorta SAX':
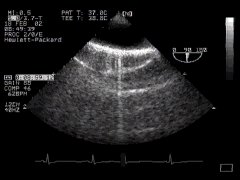
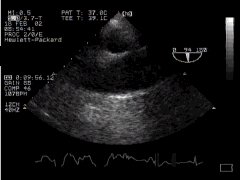
If we wish, we can view the aorta in long axis by rotating the biplane or multiplane probe through ninety degrees - 'DESC Aorta LAX':
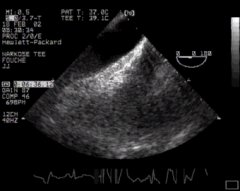
2. Aortic ArchReturning the probe to the short axis view (0o) and widthdrawing it slowly, we eventually cut the aortic arch. It's easy to see that despite the plane of the probe being 0o, we will visualise the arch as an oblong structure - we are effectively visualising the "long axis" of the arch - 'Aortic Arch LAX'. Note that as we move more proximally, the trachea becomes interposed, and we lose the arch and vessels coming off it.
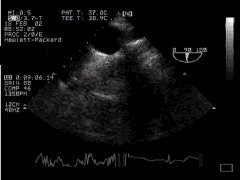
We can now rotate the probe to 90o to obtain another view of the arch, thus - 'Aortic Arch SAX':
3. Aortic RootTo visualise the proximal aorta (together with its close neighbour, the pulmonary artery) we advance the probe again past the level of the arch, and rotate it slightly to the right. Here's the short axis view, which you saw previously when we examined transverse basal views.
.. and finally, the long axis - 'ME Asc Aortic LAX':
|